Approaches to Changing Military Health Care

CBO examined possible changes to the Department of Defense’s Military Health System, analyzing the effects of those changes on the federal budget, the quality of military health care, and preparedness for wartime missions.
Summary
The Department of Defense (DoD) provides health care through its Military Health System (MHS), an organization that oversees the delivery of health care at home and abroad through a program known as TRICARE. The two primary purposes of that system are to ensure that service members are healthy enough to deploy (sometimes called medical readiness) and that military clinicians and other providers are adequately trained to care for personnel during both peacetime and wartime (sometimes called operational readiness.) A third function of the MHS is to provide health benefits as an additional form of compensation for military personnel and eligible retirees. DoD spends about $50 billion annually on the MHS.
Policymakers and analysts have raised concerns about DoD’s rising health care costs, the quality of care provided at its facilities, and how well the department’s medical establishment prepares for wartime missions. Efforts to change the system are complicated, however, partly because the resources used to accomplish the various goals are often intermingled or unclear. For this report, CBO examined several broad, illustrative approaches that might address policymakers’ concerns. In addition, the agency estimated the costs of two options that have been proposed specifically to make changes to TRICARE.
How Does DoD Provide Health Care?
The MHS provides direct care through its own system of clinics and hospitals—both in combat settings and at military installations that can be visited by TRICARE beneficiaries. It also purchases care from civilian providers by means of regional contracts. Within the United States, direct care accounts for about 40 percent of care provided through the MHS, and purchased care for the remaining 60 percent.
The following groups of people are eligible to participate in TRICARE (with the respective populations at the beginning of 2016 shown in parentheses):
- All members of the four military branches, including members of the National Guard and reserves, as well as members of the Coast Guard and the commissioned corps of the Public Health Service and of the National Oceanic and Atmospheric Administration (1.9 million);
- Families of current uniformed service members (2.0 million); and
- Military retirees and their families (5.4 million).
In general, care received at military treatment facilities (MTFs) is free for participants. For care by contract providers, participants face deductibles and other cost-sharing requirements that vary, depending on the type of plan they select, but those amounts are usually less than required by civilian health plans. In most cases, TRICARE beneficiaries pay just a small fee or premium, if any, for that coverage.
What Broad Approaches Might Improve How Health Care Is Supplied or Funded?
CBO examined three broad approaches and two specific options that would change the way DoD provides or funds health care. The approaches would fundamentally change how health care is supplied but would not focus on what beneficiaries pay for care or the effects of those costs on the demand for health care. Each of the approaches has the potential to directly or indirectly reduce costs, improve the quality of care, or improve operational readiness (or at least more clearly identify the costs of ensuring readiness). But because the costs or savings of those approaches would depend on many programmatic details, CBO did not estimate savings that might result from implementing them.
Approach 1: Focus the Direct Care System on Operational Readiness
Under this approach, the system would focus on providing care to service members and on training military clinicians and other providers. Most care provided to families and retirees would be outsourced to the private sector, substantially reducing the size of the direct care system. The effect on federal spending would depend on whether DoD was able to eliminate excess capacity (facilities, equipment, and clinical personnel no longer needed to treat families and retirees) and whether private-sector care proved to be more or less costly than direct care.
Approach 2: Pay Fixed Amounts per Person to TRICARE Contractors
This approach would give contractors more latitude to restructure provider networks, reimburse providers, and determine patients’ cost sharing. Such a transformation could save DoD money, but MTFs would need to be restructured or closed and patients would probably need to pay a larger share of their costs to generate significant savings.
Approach 3: Change the Way That Military Departments Pay for Health Care in MTFs
In general, each military department (Army, Navy, and Air Force) currently manages its own MTFs and controls its own medical operations in the wartime theater. This approach could take one of two possible forms. One would involve paying fixed amounts per beneficiary to MTFs for health care services. Another would use an internal pricing mechanism—known as a working capital fund—for military departments to purchase care in MTFs for their beneficiaries. The goal of each change would be to better distinguish the costs of providing health care from the costs of ancillary activities related to ensuring medical and operational readiness. (Ancillary activities include functions conducted at medical command headquarters, the education and training of medical personnel, and veterinary services, including the care of working animals.) Decisionmakers within DoD and the Congress could better allocate resources if those costs were known.
What Would Be the Effects of Two Specific Options?
CBO analyzed two options that have been proposed to make changes to the MHS. Earlier work by CBO found that people using military health services pay a lower share of their health care costs than most civilians with employment-based coverage. Those lower costs encourage people to switch to TRICARE and to use health care services more than comparable civilians. In CBO’s judgment—which is informed by the agency’s earlier work—policy changes that would increase beneficiaries’ cost sharing have the greatest potential to generate significant savings for DoD and the federal government as a whole. Both options were assumed to go into effect in January 2020.
Option 1: Increase Cost Sharing for Most Beneficiaries Who Use TRICARE
This option would keep the current structure of TRICARE and the Military Health System intact but would increase the out-of-pocket costs paid both by active-duty TRICARE users who wish to buy coverage for their families and by users who have retired from the military but are not yet eligible for Medicare (sometimes called working-age retirees, they are generally between the ages of 40 and 65). Under the option, savings would accrue directly to the government because beneficiaries would use fewer health care services. Savings would also be generated when beneficiaries switched to a cheaper TRICARE plan or to other sources of health insurance. Consequently, the option would primarily affect the demand for, rather than the supply of, health care.
Option 2: Replace TRICARE With a Choice of Commercial Insurance Plans for Most Beneficiaries
This option, which is based on reforms proposed by the Military Compensation and Retirement Modernization Commission, would offer commercial insurance and incorporate MTFs into those networks. It would substantially restructure the TRICARE benefit and its delivery system, including adding new cash allowances for families of active-duty personnel and raising out-of-pocket costs for working-age retirees. The option would change the supply side of the market as well as the demand side.
Effects of the Options
CBO assessed the effects of these options in the “steady state”—that is, when the policy changes would be fully implemented, which CBO projects would happen by 2031. If lawmakers reduced discretionary funding accordingly, the net effect of the options on the deficit would be an annual decrease of roughly $2.5 billion under Option 1 or an annual increase of $700 million under Option 2 (evaluated at the midpoint of the likely range of outcomes, in 2017 dollars). (See figure below.) The first option would, on net, decrease costs to DoD and other agencies by $2.9 billion per year (in 2017 dollars) but would cause a small ($0.4 billion) net increase in the deficit from reduced tax revenues and greater mandatory spending (mostly the former). By contrast, the second option could result in a small ($0.2 billion) annual decrease in discretionary costs and a slightly larger increase in the deficit ($0.9 billion) from reduced revenues (and a small change in mandatory spending.)
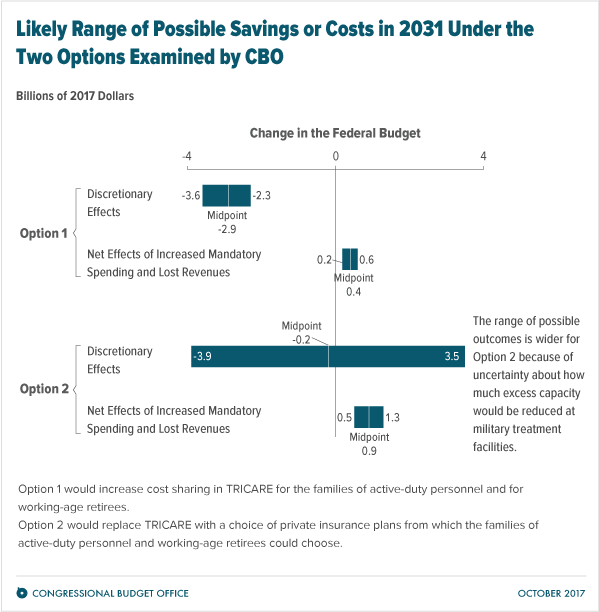
The estimated effects of Option 2 on discretionary costs are highly uncertain, however, largely because incorporating military treatment facilities and providers into commercial insurance networks would bring significant changes to beneficiaries and DoD and thus could be very difficult to implement. In particular, if operations at military treatment facilities could not be fully funded by reimbursements for providing care, any excess capacity would need to be reduced or subsidized by DoD through appropriations. The greatest uncertainty associated with the estimates for Option 2 involves the extent to which DoD would reduce any excess capacity in the Military Health System as a result of the lower demand for health care at those facilities.
Evaluating the two options on a per-family basis provides additional insights. In 2031, the first year in which the full budgetary effects of both of the options would occur, implementing Option 1 or Option 2 would result in lower annual costs to the government—by about $2,000 or $600, respectively, per retiree family. But under Option 2, that family’s out-of-pocket costs would more than triple, from about $1,900 per year to about $7,500 per year.
For an average active-duty family, the cost to the government would decrease slightly under Option 1 but increase substantially under Option 2, CBO estimates. That increase would occur in part because of the allowances paid to those families, but primarily because TRICARE prices would no longer be constrained by Medicare rates and because subsidies would be required if DoD maintained excess capacity in its military treatment facilities.